TL;DR
HIPAA-first architecture, FHIR integration, AI guardrails, real cost bands, and the compliance checklist for shipping a healthtech MVP in 8-14 weeks. From a team that has done it.
TL;DR: A HIPAA-compliant healthtech MVP costs $10,000 to $50,000 for a standard build and $30,000 to $200,000 for complex telehealth or EHR-integrated platforms, shipping in 8 to 14 weeks. Compliance is architecture, not paperwork: encryption (AES-256, TLS 1.3), MFA, audit logging, RBAC, and a signed Business Associate Agreement (BAA) with every vendor that touches PHI. We have shipped healthtech products on AWS HIPAA, integrated with HL7 FHIR R4, and passed first-attempt audits at MarsDevs. Build compliance into week one or rebuild later.
Most healthtech MVPs do not die because the engineering was bad. They die because founders treated HIPAA, BAA, and PHI as paperwork to schedule for "after launch." By the time a hospital pilot, an investor due diligence, or a SOC 2 questionnaire arrives, the architecture cannot answer for itself, and a six-month rebuild lands in the middle of the runway.
You have a healthtech idea. Maybe it is a telehealth platform on Twilio Verify, a patient intake tool that exports to Epic, or an AI scribe for primary care. The clinicians say yes. The pain point is real. The global digital health market hit $491 billion in 2026, according to Fortune Business Insights, and AI-enabled medical devices crossed 1,250 FDA authorizations as of 2025 per the FDA's public database.
Then comes the wall: 76% of healthtech MVPs that miss launch dates miss them on compliance, not features. Founders build features first, retrofit HIPAA, and discover their entire data layer needs a rebuild. That is three to six months of burned runway.
MarsDevs is a product engineering company that builds AI-powered applications, SaaS platforms, and MVPs for startup founders. Founded in 2019, we have shipped 80+ products across 12 countries, including healthcare platforms that handle PHI across telehealth, patient engagement, and clinical workflow automation. The pattern that wins every time: founders who design for HIPAA, FHIR, and BAAs in week one ship faster, spend less, and pass audits without rework.
This guide is the framework. Every compliance requirement, architecture decision, vendor question, and cost factor that matters for healthtech MVP development in 2026, with the MVP basics layered with what makes healthcare different.
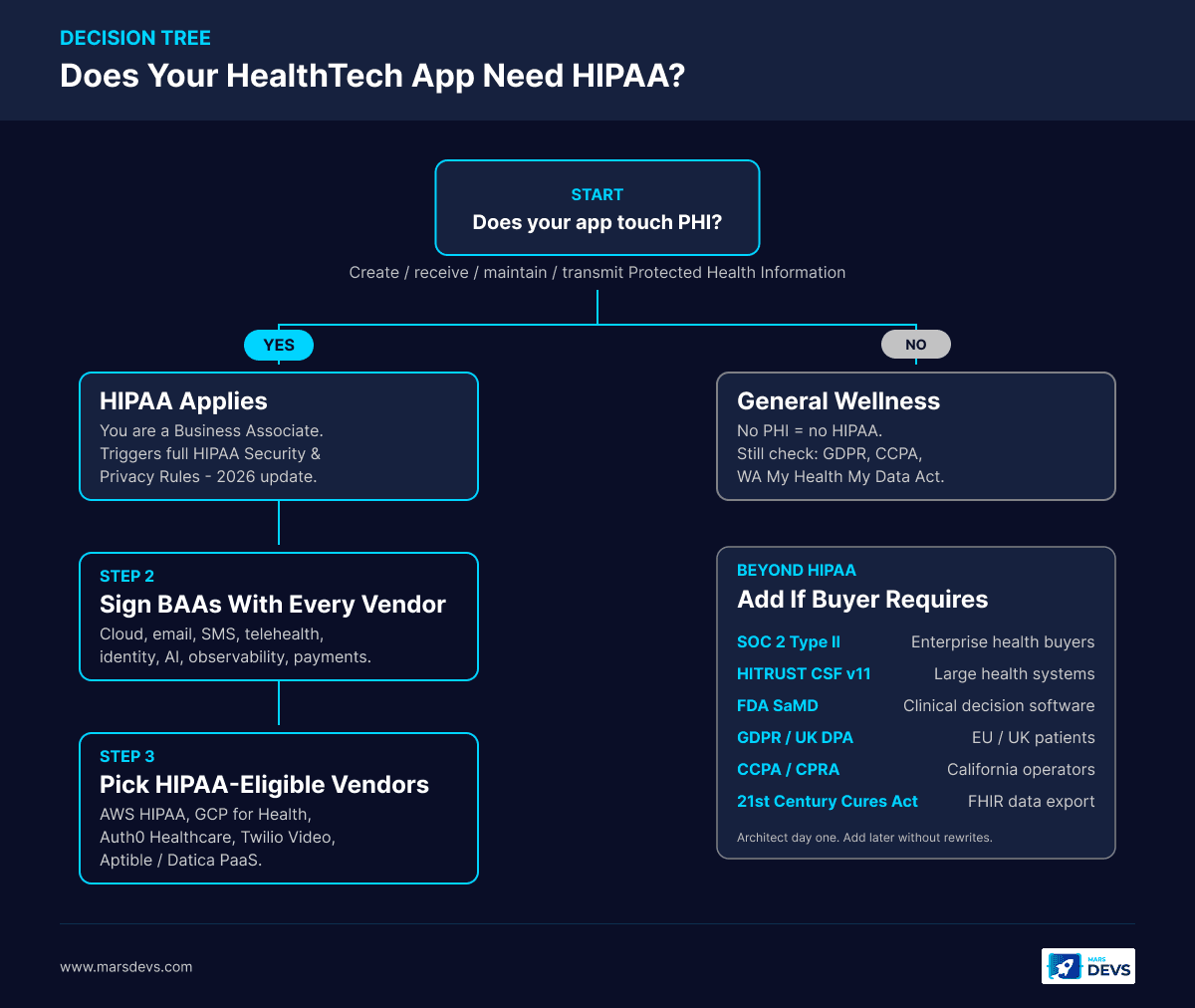
Not every health app needs the same compliance ceiling. A meditation timer, a wearable companion, and a platform that stores lab results live under three different regulators. Before you write a line of code, answer one question: does your app create, receive, maintain, or transmit Protected Health Information (PHI) on behalf of a covered entity?
HIPAA applies the moment your application touches PHI on behalf of a covered entity (hospital, clinic, payer, provider). If your app stores patient names alongside medical data, processes insurance claims, integrates with EHR systems like Epic or Cerner, or transmits clinical messages, you are almost certainly a Business Associate. That triggers the full HIPAA Security and Privacy Rules.
The 2026 HIPAA Security Rule update closes every "addressable" loophole. Encryption and multi-factor authentication (MFA) are now mandatory for all systems that process electronic PHI (ePHI), per HIPAAVault's 2026 update guidance. If you are building a healthtech MVP today, design for the new rule, not the old one.
| Your App Does This | HIPAA Required? | Why |
|---|---|---|
| Stores patient records or lab results | Yes | Directly handles PHI |
| Integrates with EHR/EMR systems via FHIR | Yes | Receives PHI from covered entities |
| Processes insurance claims or billing codes | Yes | Handles identifiable health data |
| Provides telehealth video consultations | Yes | Transmits PHI in real time |
| Sends appointment reminders with names + visit type | Yes | Names + clinical context = PHI |
| Tracks fitness data without linking to medical records | No (usually) | General wellness, not PHI |
| Offers symptom checking with no patient identification | No (usually) | No identifiable health data stored |
| Stores wearable heart rate exported into a clinical chart | Yes | Once it lands in the chart, it is PHI |
HIPAA is the baseline, not the ceiling. Depending on your product, market, and buyer, you may also need:
For your MVP, focus on HIPAA first. Architect so SOC 2 Type II and HITRUST i1 can be added later without a rewrite. Founders weighing whether to build custom or buy off the shelf usually find healthtech is one of the clearest custom-build cases. Generic platforms cannot match the audit, BAA, and FHIR requirements specific buyers will demand. Read our take on tech stacks for startups in 2026 for how this pairs with broader stack choices.
This is the checklist we use on every healthtech project at MarsDevs. It covers technical safeguards, administrative requirements, and vendor obligations your MVP needs before it touches patient data.
The 2026 HIPAA Security Rule makes all of these explicit, no longer "addressable":
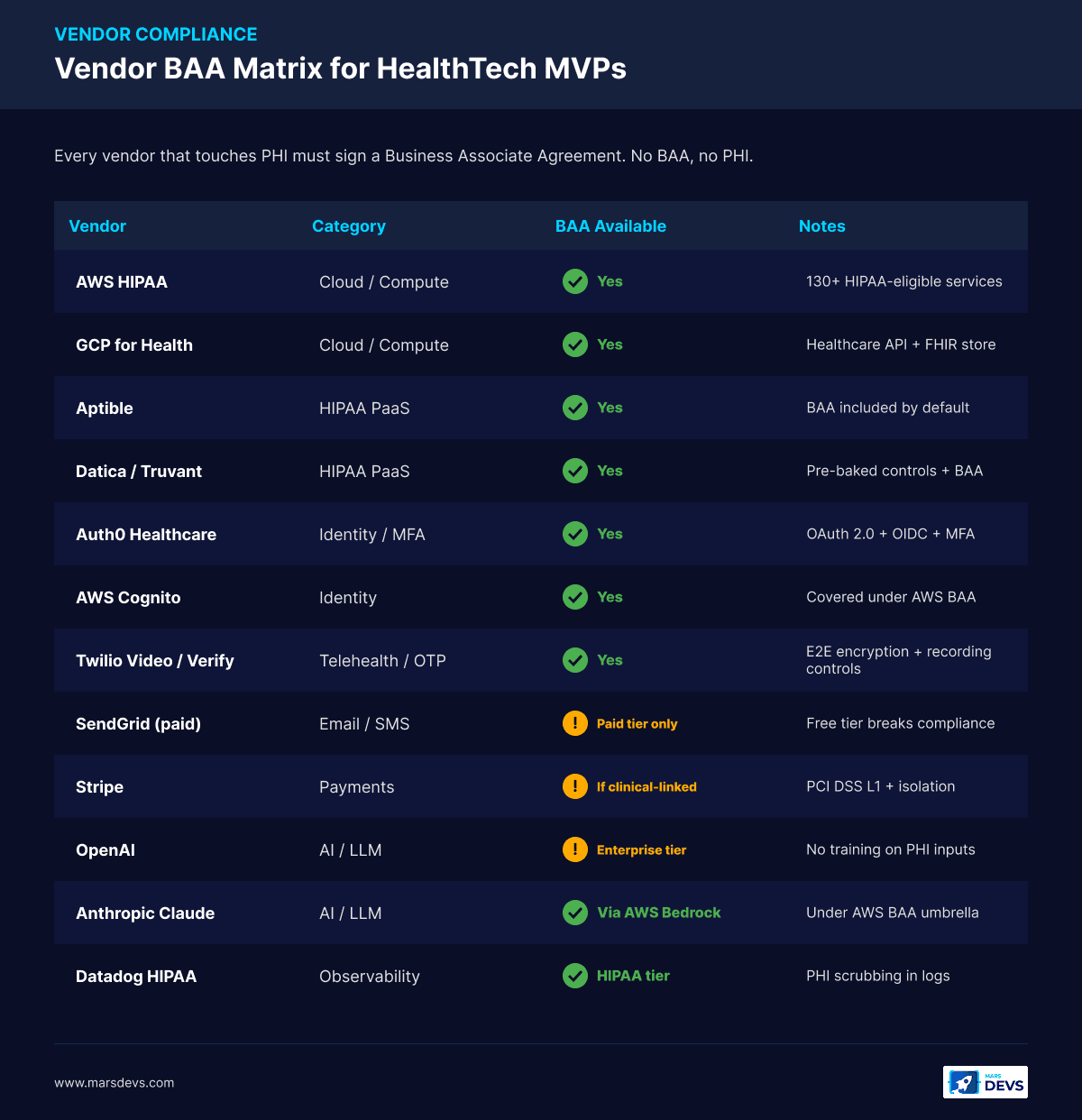
Your app is only as compliant as the weakest vendor in your stack. We have seen single-vendor gaps invalidate entire compliance postures:
| Vendor Type | BAA Required? | What to Verify |
|---|---|---|
| Cloud hosting (AWS, GCP, Azure) | Yes | HIPAA-eligible service list, encryption defaults, CloudTrail/Audit Logs enabled |
| Database (RDS, Cloud SQL, MongoDB Atlas) | Yes | Encryption at rest, TLS in transit, point-in-time recovery, retention |
| Email/SMS (SendGrid, Twilio, AWS SES) | Yes (if PHI sent) | Signed BAA, TLS-only delivery, no PHI in subject lines |
| Telehealth SDK (Twilio Video, Vonage, Zoom for Healthcare) | Yes | End-to-end encryption, recording consent, U.S./EU data residency |
| Identity (Auth0, AWS Cognito, Okta) | Yes | Auth0 Healthcare or Cognito with BAA, MFA enforced, session controls |
| Analytics/observability (Datadog, Sentry) | Yes (if logs contain ePHI) | PHI scrubbing, log access controls, BAA on file |
| AI providers (OpenAI, Anthropic, Google, AWS Bedrock) | Yes | OpenAI Enterprise BAA, Anthropic via AWS Bedrock with AWS BAA, no training on inputs |
| Payment (Stripe, Adyen) | Yes (if linked to clinical data) | PCI DSS Level 1, data isolation, BAA where required |
| HIPAA-native PaaS (Aptible, Datica, Truvant) | Yes (built-in) | Pre-configured controls, BAA included, faster go-to-market |
A common founder mistake we see at the kickoff: a free-tier SendGrid plan sending appointment reminders with patient names and visit types. That single vendor gap makes the entire app non-compliant, even if every server is encrypted. Audit your vendors before you audit your code.
Compliance shapes architecture before a single feature decision is made. Here are the patterns that pass audits and scale into v2 without rebuilds. They are the patterns we standardize on internally at MarsDevs and they map cleanly to the broader SaaS architecture playbook we use across non-healthcare builds.
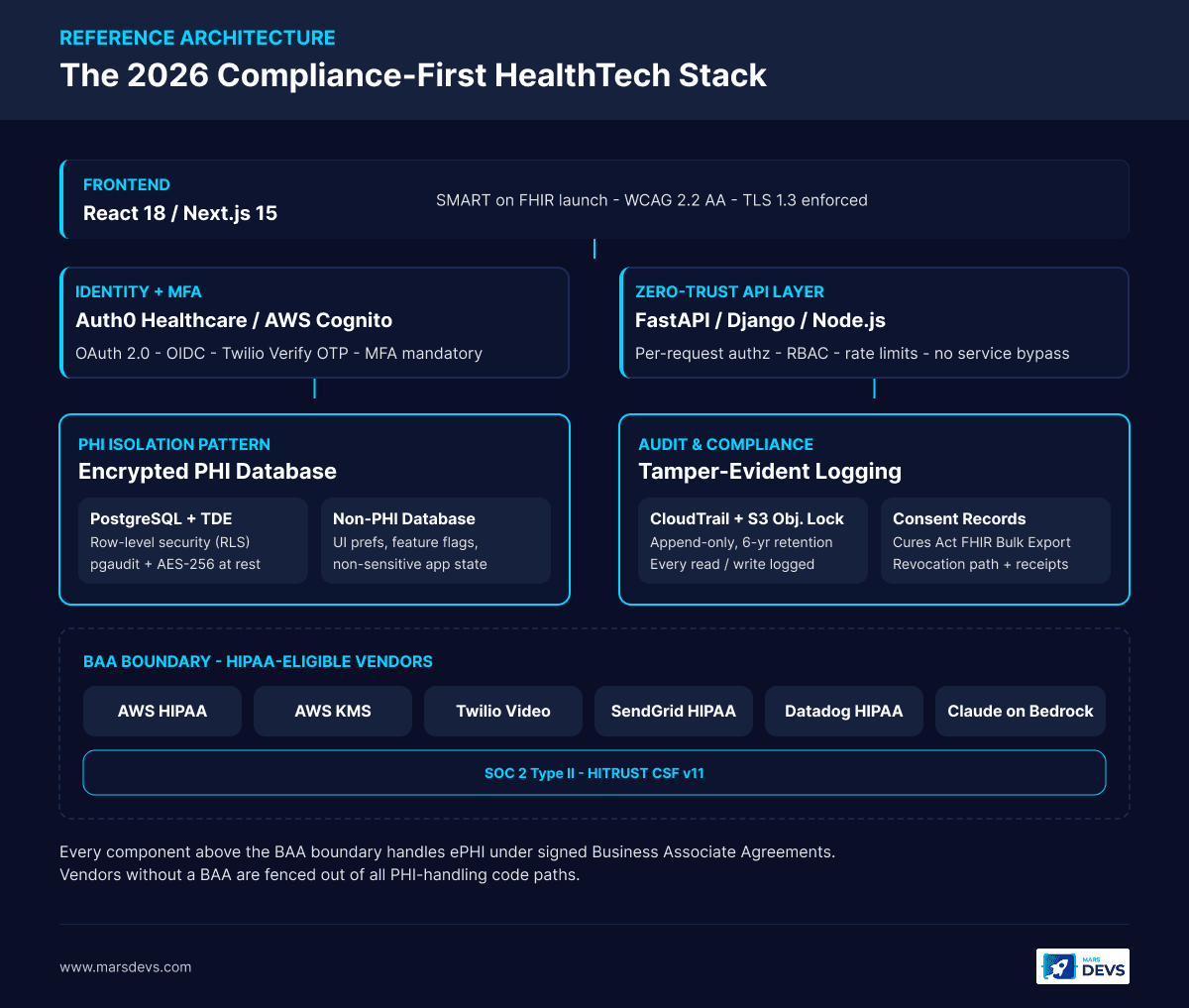
After shipping healthcare products across telehealth, patient intake, and clinical workflows, we converge on a stack that balances velocity with audit-readiness:
| Layer | Recommended | Why |
|---|---|---|
| Frontend | React 18 or Next.js 15 | Component-based UIs make accessibility (WCAG 2.2 AA) and SMART on FHIR integration easier. |
| Backend | Python (FastAPI or Django) or Node.js | Python wins when AI is on the roadmap; the FHIR library ecosystem (fhir.resources, HAPI FHIR) is mature. |
| Database | PostgreSQL with TDE + row-level security | Battle-tested, supports RLS, strong audit trail extensions (pgaudit). |
| Cloud | AWS HIPAA-eligible services or GCP for Health | Both offer BAAs, granular IAM, KMS-managed keys, CloudTrail/Audit Logs. AWS for Health is the most common starting point. |
| Auth | Auth0 Healthcare, AWS Cognito (with BAA), or Okta | OAuth 2.0 + OIDC + MFA. Twilio Verify for OTP. Never roll custom auth for healthtech. |
| FHIR | HAPI FHIR (Java) or fhir.resources (Python) | Handles HL7 FHIR R4 parsing, validation, serialization, and SMART app launch. |
| Telehealth | Twilio Video, Vonage, Zoom for Healthcare | All offer BAAs, end-to-end encryption, and clinical-grade recording controls. |
| HIPAA PaaS (optional) | Aptible, Datica, Truvant | Pre-baked controls accelerate first audit. We pick this for solo founders without DevOps. |
| Observability | Datadog HIPAA, AWS CloudWatch + GuardDuty | PHI scrubbing in logs, BAA-covered metrics. |
Patient data needs a different architecture than typical SaaS. If you have built standard web apps before, expect structural shifts.
1. PHI Isolation Pattern. Store PHI in a separate, encrypted database or schema from non-sensitive application data. Limit blast radius and simplify audit scope. User preferences, UI state, and feature flags live in one database. Patient health records live in another with stricter access controls, separate KMS keys, and tighter IAM policies. We default to this pattern on every healthtech project.
2. Zero-Trust API Layer. Every API call that touches PHI goes through an authentication and authorization layer with no service-to-service bypass. Every request is logged with the requesting principal, the resource accessed, and the action performed. This adds 5 to 10ms of latency per call but produces a complete, immutable audit trail that satisfies HIPAA auditors and SOC 2 reviewers.
3. Consent-First Data Flow. Before any PHI is collected, processed, or shared, verify and record patient consent. Store consent records with timestamps, the data categories authorized, the purpose of collection, and the revocation path. The 21st Century Cures Act requires patients to access their data through standardized APIs. Build data export from week one, not as a phase-2 retrofit.
If your healthtech MVP needs to pull or push data to electronic health records (Epic, Oracle Cerner, Allscripts/Veradigm, athenahealth, MEDITECH), HL7 FHIR R4 is your integration standard. The 21st Century Cures Act and the ONC Information Blocking Rule made FHIR the legal standard for U.S. healthcare data exchange. According to a 2024 HIMSS report, 78% of healthcare providers using FHIR experienced faster care coordination compared to legacy HL7 v2 interfaces.
Here is what FHIR integration looks like at the MVP stage:
For deeper coverage of building AI-powered MVPs with complex integrations, see our guide to building an AI MVP.
Building a healthtech MVP and want an engineering team that has done this before? Talk to our engineering team.
AI is the growth engine of healthtech in 2026. The FDA has authorized over 1,250 AI-enabled medical devices, with 295 new clearances in 2025 alone. For AI development cost ranges and broader AI MVP planning, see our companion guides. The use cases are real, but AI in healthcare carries failure modes that do not exist in e-commerce or fintech.
These are the AI use cases gaining traction in healthtech MVPs right now:
The safest entry point for an AI-powered healthtech MVP is administrative automation or clinical decision support. These create clear ROI, operate as decision-support tools (not autonomous decision-makers), and face lighter regulatory scrutiny than diagnostic AI.
A chatbot that hallucinates in an e-commerce app causes a bad customer experience. A chatbot that hallucinates in a clinical setting can cause patient harm. The guardrails are different in kind, not just degree.
MarsDevs provides senior engineering teams for founders who need to ship fast without compromising quality. When we build AI-powered healthtech, we design the guardrail infrastructure alongside the AI features, not after them. Every AI component gets an evaluation framework that measures accuracy, bias, and failure modes before it touches real patient data.
Founders ask us two questions: how much, and how long. Here are the ranges we use, anchored to MarsDevs engagement pricing.
| Tier | Cost Range | Timeline | What You Get |
|---|---|---|---|
| Lean HealthTech MVP | $10,000 to $25,000 | 6 to 8 weeks | Single-workflow web app, HIPAA basics on a HIPAA PaaS (Aptible/Datica), basic PHI handling, no EHR integration, hosted infrastructure |
| Standard HealthTech MVP | $25,000 to $50,000 | 8 to 12 weeks | Patient or provider workflow, HIPAA-eligible AWS, BAA paperwork done, telehealth or one EHR read-only integration via FHIR, mobile-responsive web, admin dashboard, audit logging |
| Complex HealthTech / Enterprise | $50,000 to $200,000 | 12 to 24 weeks | Multi-provider platform, full FHIR read/write, AI feature with guardrails, SOC 2 Type II preparation, native iOS/Android, analytics, multi-region availability |
These ranges align to MarsDevs' official engagement pricing and our developer rate of $15 to $25 per hour. Compare with our SaaS build cost ranges and our last 5 SaaS builds breakdown for non-healthcare baselines. Healthtech pricing sits at the upper end of comparable SaaS work because of the compliance overhead.
If you have been burned by a dev shop that quoted half this and then missed every deadline, you are not alone. Healthtech has zero room for cut-rate compliance work. The rework always costs more than doing it right. For broader cost-to-build context, see our MVP development cost guide.
HIPAA compliance adds 30 to 50% to a comparable non-healthcare MVP budget, according to multiple industry estimates. The breakdown we typically see on healthtech projects:
Budget for these recurring expenses:
The biggest cost mistake we see: choosing a development partner on the lowest bid, then paying twice when the product fails an audit. We staff senior engineers at $15 to $25 per hour, which means founders get compliance expertise without enterprise agency rates.
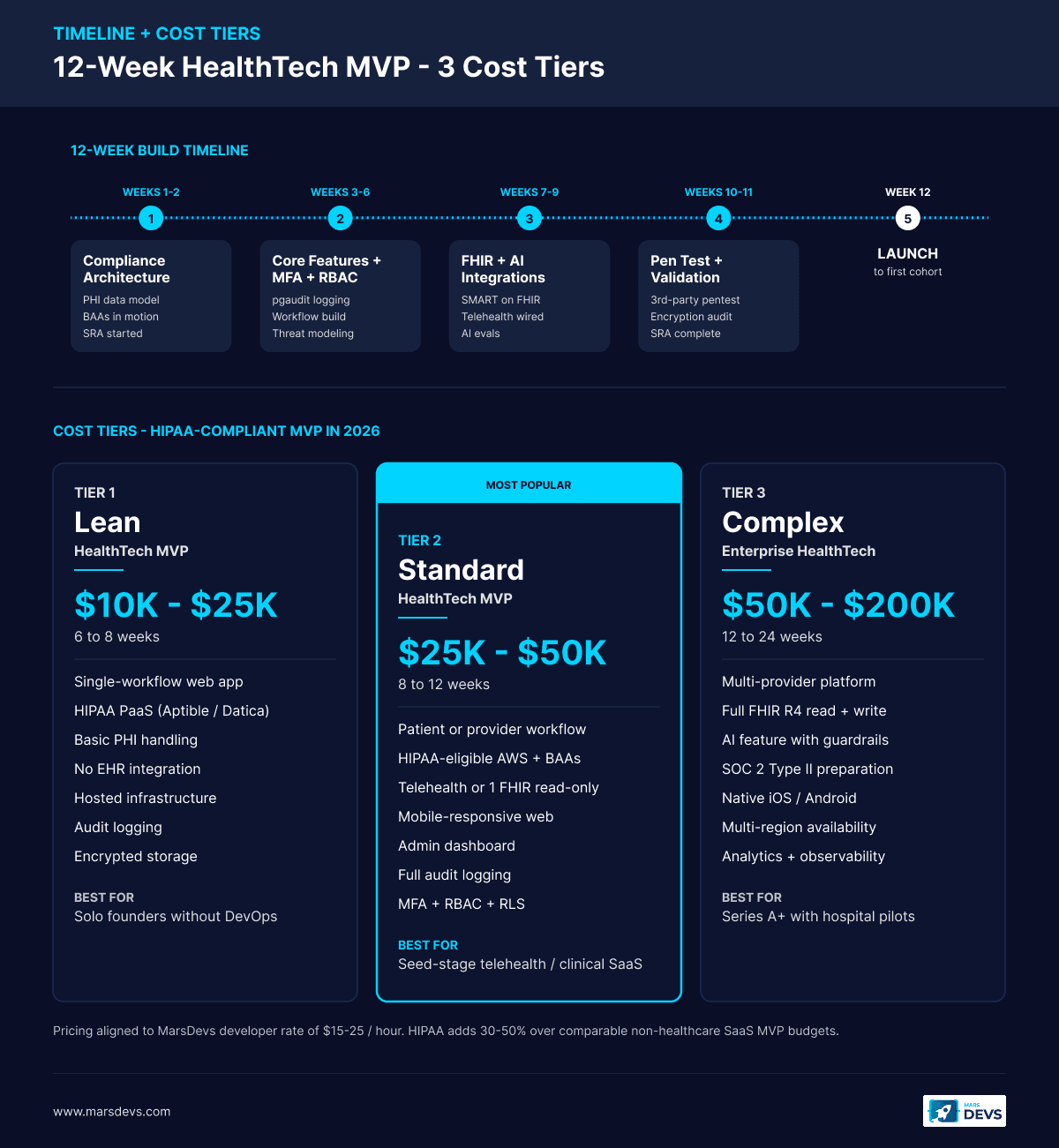
Speed matters in healthtech. Not reckless speed: disciplined speed. Here is the 12-week timeline we use for standard healthtech MVP development.
Define your PHI data model. Map regulatory requirements (HIPAA scope, SOC 2 horizon, FDA classification, GDPR if applicable). Select HIPAA-eligible vendors. Sign BAAs with cloud, identity, telehealth, AI, and observability providers. Stand up encrypted infrastructure on AWS HIPAA-eligible services or a HIPAA PaaS. Set up CI/CD with secret scanning, dependency scanning, and IaC validation. Start the formal Security Risk Analysis.
Build the primary patient or provider workflow. Implement Auth0 Healthcare or Cognito with MFA, RBAC at the row and column level, and pgaudit-backed audit logging. Every feature ships with its compliance components built in (logging, access checks, consent records), not bolted on separately. Run weekly internal threat modeling on new endpoints.
Connect to EHR sandboxes via SMART on FHIR. Validate FHIR R4 resource parsing for Patient, Observation, MedicationRequest, AllergyIntolerance, and DocumentReference. Build and test any AI features with evaluation frameworks. Implement consent management UI and patient data export endpoints (Cures Act readiness). Wire telehealth (Twilio Video or Vonage) end-to-end.
Run a third-party penetration test. Validate encryption (at rest, in transit, key rotation), access controls, MFA enforcement, session timeouts, and audit logs against the HIPAA checklist. Fix every finding. Complete the Security Risk Analysis. Draft incident response and breach notification runbooks.
Final compliance review with a healthcare attorney. Incident response tabletop exercise. Monitoring, alerting, and on-call rotation configured. Backup and disaster recovery drill. Deploy to production behind a feature flag and roll forward to first patient cohort.
We start building within 48 hours of project kickoff. For healthtech, those first two days focus on infrastructure and paperwork: encrypted environments, BAA paperwork in motion, and CI/CD with automated security checks. Features come after the compliance foundation is solid.
Lived experience matters more than playbook in healthcare. Three patterns from MarsDevs healthtech work that hold up:
The pattern across all three: compliance is architecture, the BAA boundary is sacred, and human-in-the-loop is the AI guardrail that keeps you on the safe side of the FDA.
Three out of four healthtech MVPs that come to us for a rebuild repeat the same mistakes. Catching these before week one saves six figures and six months.
The most expensive mistake is wiring "HIPAA mode" into a generic SaaS architecture: a single multi-tenant Postgres for all data, app-level encryption, and a hope that BAAs cover the gaps. By the time a hospital security questionnaire arrives, the data layer cannot answer questions about minimum-necessary access, audit completeness, or breach blast radius. Rebuilds at this stage typically run 60% of the original budget, plus three months of lost go-to-market.
The fix is the PHI isolation pattern from week one: a dedicated PHI database, a separate KMS key per environment, RBAC enforced at the row and column level via Postgres row-level security, and pgaudit logs piped to a write-once store. This is the same architecture we use across our SaaS architecture for startups work, hardened for HIPAA.
Founders often assume vendor BAAs are paperwork that can wait. They cannot. A free-tier observability tool, an analytics SDK, a support inbox, or a non-HIPAA email provider can each invalidate compliance the day the first PHI touches them. We have seen launches blocked at week 11 of a 12-week build because a Slack bot was forwarding error messages with patient identifiers.
The fix is a BAA inventory in week one. Every vendor in the stack gets a row: name, what they touch, BAA status, BAA contract link, fallback if no BAA. Anything without a BAA is either swapped (Sentry to a HIPAA-tier observability stack, free SendGrid to a paid HIPAA-eligible plan) or fenced out of all PHI-handling code paths.
Healthcare is the worst category in which to roll your own auth, your own MFA, or your own encryption. The compliance risk dwarfs the savings. Use Auth0 Healthcare, AWS Cognito with a BAA, or Okta. Use AWS KMS or GCP Cloud KMS for keys. Use TLS 1.3 from a managed load balancer, not a hand-rolled certificate stack. Every hour spent reinventing these primitives is an hour not spent on the patient-facing differentiation that wins pilots.
Founders typically assume Epic or Cerner integration is a 2-week task. Sandbox integration is. Production credentials are not. App registration with Epic on FHIR or Oracle Health Developer Network can take 4 to 12 weeks depending on scope, certification, and the partner health system's onboarding queue. Start the application during week 1, not week 9. Read-only FHIR access is the fastest path to a green light.
HIPAA-only thinking misses California's CPRA, Washington's My Health My Data Act, and the federal 21st Century Cures Act information-blocking rules. Patient data export endpoints, consent receipts, and category-specific privacy notices are not optional for U.S. operators with multi-state footprints. Build a GET /patient/{id}/export FHIR Bulk Data endpoint and a consent log table from day one and these requirements stop being last-minute scrambles.
Healthcare hiring is slow. The senior backend engineer with HIPAA, FHIR, and AWS HIPAA experience that you need is competing with Doximity, Abridge, Hims, Cedar, and every digital-health Series B in the market. The average time-to-hire for a senior healthcare engineer in the U.S. ran 89 days in 2025 per industry hiring reports. That is most of an MVP timeline gone before code is written.
The case for an engineering partner like MarsDevs in healthtech is sharper than in adjacent categories. We come with the architecture playbook, the BAA inventory, the FHIR sandbox experience, and senior engineers who have shipped in this category. We also come at $15 to $25 per hour on the developer rate, which keeps compliance overhead from blowing up the budget the way enterprise agency rates would. Founders typically use us to ship the MVP, prove the market, and then layer in-house hiring on top once revenue or the next round are committed.
The case for in-house from day one is real when the founder is a clinician-engineer with deep domain experience, when the IP is the model itself (FDA SaMD pathway), or when the buyer is going to require exclusive engineering ownership in due diligence. Outside those cases, an engineering partner is usually the faster, cheaper, and lower-risk path through the first 12 to 18 months.
No. HIPAA applies only when your app creates, receives, maintains, or transmits Protected Health Information (PHI) on behalf of a covered entity such as a hospital or insurer. General wellness apps with no provider linkage usually fall outside HIPAA. The moment you connect to an EHR or store identifiable medical data, HIPAA applies.
A standard HIPAA-compliant healthtech MVP costs $25,000 to $50,000 and ships in 8 to 12 weeks. Lean MVPs on a HIPAA PaaS run $10,000 to $25,000. Complex platforms with EHR write access, AI, or SOC 2 prep run $50,000 to $200,000. HIPAA adds 30 to 50% to a comparable non-healthcare MVP budget.
The best healthtech stack is React or Next.js on the frontend, FastAPI or Node.js on the backend, PostgreSQL with row-level security, and AWS HIPAA-eligible services or GCP for Health with a signed BAA. Use Auth0 Healthcare or AWS Cognito for identity. Never roll your own auth for healthtech.
EHR integration uses HL7 FHIR R4 with the SMART on FHIR authorization framework, both legally required under the 21st Century Cures Act for certified EHRs. Start read-only against Epic, Cerner, and SMART Health IT sandboxes. Pull demographics, medications, and labs. Save full write access for v2.
Yes, with a BAA. OpenAI offers Enterprise BAAs covering GPT-4 class models. Anthropic Claude is BAA-eligible via AWS Bedrock under the AWS BAA. Always pair LLM use with human-in-the-loop review, model versioning, retrieval grounding, and audit logs of every prompt, output, and retrieval source.
At minimum, HIPAA if it handles PHI. SOC 2 Type II is increasingly required by hospital systems and enterprise buyers (6 to 12 months to achieve). HITRUST CSF maps across HIPAA, SOC 2, NIST, and ISO 27001 and is valued by large health systems. FDA SaMD applies if your software influences clinical decisions.
A lean healthtech MVP ships in 6 to 8 weeks. A standard MVP with HIPAA, telehealth or FHIR read-only, and an admin dashboard ships in 8 to 12 weeks. Complex platforms with AI, EHR write access, and SOC 2 prep run 12 to 24 weeks. Compliance-first architecture from week one is what keeps timelines honest.
A BAA is a HIPAA-required contract between a covered entity (or business associate) and any vendor that handles PHI on their behalf. Cloud (AWS/GCP/Azure), email/SMS, telehealth SDKs, identity, AI providers, observability tools, and payment processors linked to clinical data all need BAAs. No BAA, no PHI.
Building a healthtech product is not harder than building a fintech product or an AI-powered SaaS tool. It is different. The rules are stricter, the stakes involve patient safety, and the cost of getting compliance wrong is measured in lawsuits and lost trust, not just lost customers.
The founders who win in healthtech treat compliance as a feature, not a tax. They build encryption, audit logging, RBAC, and consent management into sprint one. They sign BAAs with every vendor before writing application code. They test against Epic and Cerner FHIR sandboxes before pitching to health systems. They version every AI model and keep humans in the loop on every clinical output.
Our senior engineering teams build healthtech MVPs with compliance baked into the architecture from day one: AWS HIPAA, FHIR R4, BAA-covered AI providers, and audit-ready logging. You pass audits on the first attempt and ship to patients in weeks, not quarters.
Want to build a healthtech MVP that is compliant from the first commit? Book a free strategy call with our engineering team. We take on 4 new projects per month. Claim a slot before your competitors do.
Co-Founder, MarsDevs
Vishvajit started MarsDevs in 2019 to help founders turn ideas into production-grade software. With deep expertise in AI, cloud architecture, and product engineering, he has led the delivery of 80+ software products for clients in 12+ countries.
Get more guides like this
Join founders, CTOs, and engineering leaders who receive our engineering insights weekly. No spam, just actionable technical content.
Partner with our team to design, build, and scale your next product.
Let’s Talk